If you’ve ever felt like your body is working against you, you are not imagining it. Lipedema fat does not behave the same way as typical weight gain, and that difference matters more than most women are ever told. When we understand what is actually happening in the tissue, it becomes much easier to stop blaming ourselves and start focusing on strategies that actually support the body.
Lipedema Fat Is Not “Just Weight Gain”
In typical obesity, fat tissue expands largely through a combination of existing fat cells getting larger (hypertrophy) and the creation of new fat cells (hyperplasia). In lipedema, both processes are present too, but the tissue behaves differently in ways that go well beyond simple fat accumulation.
Research has confirmed that lipedema adipose tissue shows significant adipocyte hypertrophy, with cell size increasing progressively as the condition advances through stages. There is also evidence of enhanced adipogenic differentiation, meaning lipedema fat cells may have a greater capacity to multiply and mature than typical fat cells. This helps explain why lipedema tissue can feel so different and why it does not respond to diet and exercise the way conventional fat does.
What Is Happening Beneath the Surface
Lipedema is not a surface-level or cosmetic condition. The tissue itself is structurally distinct. As lipedema progresses, several changes tend to occur in the affected tissue:
- Adipocyte size increases, particularly in areas like the thighs
- Fibrotic collagen (types I and III) accumulates within the extracellular matrix
- The tissue becomes denser, firmer, and more nodular
- Lymphatic and vascular flow can become restricted, especially in later stages
This is part of why so many women describe lipedema areas as painful, heavy, and resistant to change, even with consistent effort around nutrition and movement. It is not a willpower problem. It is a tissue biology problem.
The Role of Hormones
The hormonal connection to lipedema is significant, and it helps explain why so many women notice onset or worsening during major hormonal transitions.
Estrogen plays a central role in regulating how subcutaneous fat tissue grows and remodels. In lipedema, the balance between estrogen receptor subtypes, specifically ERα and ERβ, appears to be disrupted in ways that promote fibrosis, impair fat mobilization, and drive disordered tissue expansion. This dysregulation may also explain why lipedema often first appears at puberty, worsens during pregnancy, and frequently accelerates around perimenopause and menopause.
Estrogen signaling influences collagen gene expression and extracellular matrix remodeling directly. When this system becomes imbalanced, it contributes to the fibrotic, firm tissue texture that is characteristic of more advanced lipedema and makes the tissue increasingly resistant to conventional fat loss strategies over time.
Inflammation, Immune Signaling, and the Gut Connection
Research is also pointing to the role of gut-derived signals in lipedema tissue behavior.
One proposed mechanism involves bacterial lipopolysaccharides, or LPS, which are compounds released from gram-negative bacteria that can move from the gut into circulation when intestinal barrier function is compromised. Researchers have proposed that LPS may selectively accumulate in gluteofemoral white adipose tissue, triggering low-grade inflammation that drives further adipose expansion. This fits with the broader body of research linking metabolic endotoxemia to insulin resistance, chronic inflammation, and adipose tissue dysfunction.
This does not mean lipedema is a gut disease. But it does reinforce why a multi-system approach, one that addresses inflammation, barrier function, and metabolic signaling together, may be more effective than focusing on fat loss alone.
A Key Difference in Immune Activity
One of the most important discoveries in recent lipedema research is how immune cells behave differently in lipedema tissue compared to obesity.
In obesity, fat tissue is typically characterized by a predominance of pro-inflammatory M1 macrophages, which drive chronic inflammation and metabolic disruption.
In lipedema, the opposite pattern has been observed. The tissue shows a predominance of anti-inflammatory M2 macrophages, identifiable by high expression of the CD163 receptor. Multiple independent research groups have confirmed this finding.
This distinction matters clinically. M2 macrophages in lipedema appear to actively promote adipogenesis and tissue remodeling, meaning the immune environment in lipedema tissue may be actively driving fat cell growth and fibrosis rather than causing the kind of inflammatory damage we see in obesity. Some researchers now propose that this unique immune profile is what makes lipedema tissue so structurally distinct and so resistant to conventional fat loss approaches.
It is also worth noting that approximately half of women with lipedema also have obesity. When both are present, their effects can overlap and intensify, contributing to greater metabolic disruption, shifts in adipokines like leptin and adiponectin, and increased fibrotic burden in the tissue.
So What Does This Mean for Fat Loss?
If lipedema fat behaves differently, then the approach to supporting it needs to be different too. This is not about restriction or pushing harder. It is about supporting the systems that influence how the tissue behaves.
That includes:
- Supporting insulin sensitivity to reduce metabolic strain on the tissue
- Reducing inflammatory signaling where possible, including gut-derived contributors
- Encouraging healthy lymphatic flow and regular movement
- Supporting tissue health over time, including strategies that address fibrosis
- Considering hormonal context, especially during perimenopause and menopause
When we shift the focus this way, the conversation changes. It is no longer about blame or willpower. It becomes about physiology and support.
Take a Personalized Approach
Lipedema is complex, but understanding the biology behind it can be incredibly freeing.
When you know what is actually happening beneath the surface, you can stop trying to force your body into strategies that were never designed for it and start focusing on approaches that align with how your tissue works.
This is the foundation of what we do inside The Lipedema Method, where we focus on personalized, biology-based strategies that support insulin balance, reduce inflammation, and promote long-term tissue health.
If you are ready for an individualized approach that looks at the full picture of your body, The Lipedema Method was created for you. It takes the guesswork out and helps you build a plan that actually makes sense for your physiology.
References
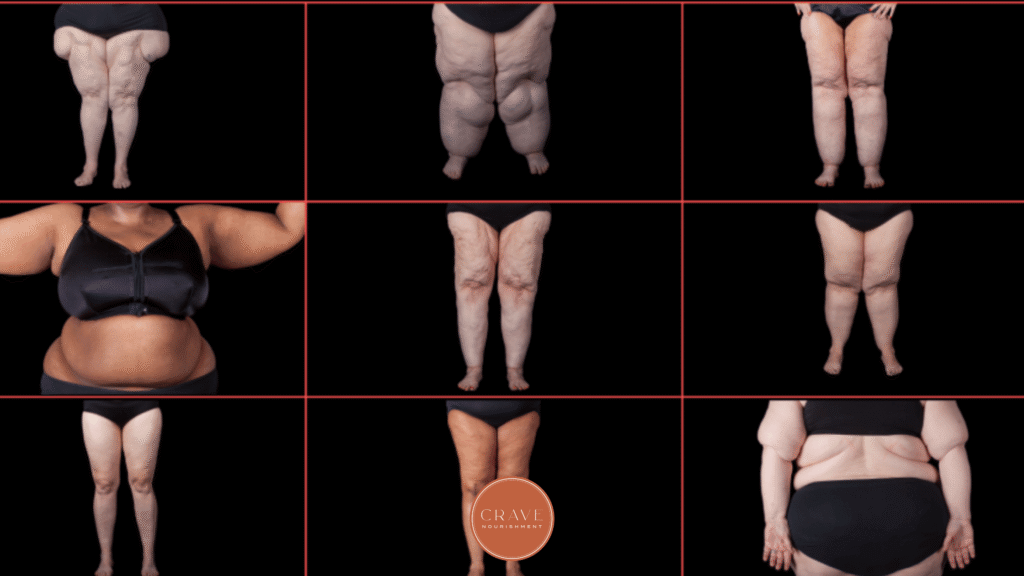
Header Image from The Lipedema Foundation
Al-Ghadban S, Cromer W, Allen M, et al. Dilated Blood and Lymphatic Microvessels, Angiogenesis, Increased Macrophages, and Adipocyte Hypertrophy in Lipedema Thigh Skin and Fat Tissue. J Obes. 2019;2019:8747461.https://doi.org/10.1155/2019/8747461
Ishaq M, Bandara N, Morgan S, et al. Key signaling networks are dysregulated in patients with the adipose tissue disorder, lipedema. Int J Obes (Lond). 2022;46(3):502-514.https://doi.org/10.1038/s41366-021-01002-1
Kruppa P, et al. Adipocyte hypertrophy, aberrant biochemical profile, and distinct gene expression in lipedema. Plast Reconstr Surg. 2020;146(5):1110-1122.https://doi.org/10.1097/PRS.0000000000007215
Wolf S, Rannikko JH, Virtakoivu R, et al. A distinct M2 macrophage infiltrate and transcriptomic profile decisively influence adipocyte differentiation in lipedema. Front Immunol. 2022;13:1004609.https://doi.org/10.3389/fimmu.2022.1004609
Grewal T, Kempa S, Buechler C. Lipedema: A Disease Triggered by M2 Polarized Macrophages? Biomedicines. 2025;13(3):561.https://doi.org/10.3390/biomedicines13030561
Straub RH, et al. Lipedema and adipose tissue: current understanding, controversies, and future directions. PMC. 2025.https://pmc.ncbi.nlm.nih.gov/articles/PMC12631410/
Duhon B, et al. Is the endotoxin-complement cascade the major driver in lipedema? Med Hypotheses. 2024.https://doi.org/10.1016/j.mehy.2024.111367
Frontiers in Cell and Developmental Biology. New Frontiers in modeling the lipedema microenvironment in vitro. 2026.https://doi.org/10.3389/fcell.2026.1816014
Bicca J. Menopause as a Critical Turning Point in Lipedema: The Estrogen Receptor Imbalance, Intracrine Estrogen, and Adipose Tissue Dysfunction Model. Preprints. 2025.https://doi.org/10.20944/preprints202506.1813.v1
Unraveling lipedema: comprehensive insights and the path to future discoveries. npj Metab Health Dis. 2026.https://doi.org/10.1038/s44324-025-00093-y

